The Z Machine
Footballguy
GLLLLLL, IK.
I walked into the HCA Florida Blake Hospital in Bradenton Fl to pick up a friend and when i walked in they had a box of masks on the reception counter. I noticed the 2 people behind the counter were in fact NOT wearing masks , so i asked if masks were optional and they yes , i further inquired ,''so i dont have to wear a mask?'' ,they said absolutely not .I've made my views on masking very clear and even I don't have any serious objection to hospitals requiring masks. (I'd prefer that they didn't, but I get it).
It was 102 before I took Tylenol and passed out for the night. Will test again. Maybe it’s a flu thing. Just weird timing.Sounds odd for covid. How high was your fever?I had the worst acid reflux and heartburn of my life last night. Couldn’t sleep at all and then slept from 9am to 2pm. Low fever, headache and am totally wiped out now. Negative for covid this afternoon but I have a bad feeling about this.
 yourlocalepidemiologist.substack.com
yourlocalepidemiologist.substack.com
Another big change is that most unvaccinated individuals may now receive a single dose of a bivalent vaccine, rather than mutiple doses of the original single-strain vaccines, the agency said. The FDA simplified its recommendation for unvaccinated individuals after recognizing that most Americans now have some immunity against Covid-19, even if its just through past infections.
“Evidence is now available that most of the U.S. population 5 years of age and older has antibodies to SARS-CoV-2, the virus that causes COVID-19, either from vaccination or infection that can serve as a foundation for the protection provided by the bivalent vaccines. COVID-19 continues to be a very real risk for many people, and we encourage individuals to consider staying current with vaccination, including with a bivalent COVID-19 vaccine. The available data continue to demonstrate that vaccines prevent the most serious outcomes of COVID-19, which are severe illness, hospitalization, and death,” said Dr. Peter Marks, head of FDA’s Center for Biologics Evaluation and Research, in a news release.
I forget who said it now... It wasn't YLE, maybe Topol? At any rate that person and a group of other docs/epidems were interviewed and after discussion they said the chances of another Omicron level event in the next 2-5 years was ~20%.A society-changing variant causing a super super-spike in cases and infirmity and this truly affecting everyday life in the U.S.? Really hard to see how that can happen again in the near future. Yes, even with 2020-22 firmly in mind. Yes, even considering Delta and Omicron.
 erictopol.substack.com
erictopol.substack.com
At any rate that person and a group of other docs/epidems were interviewed and after discussion they said the chances of another Omicron level event in the next 2-5 years was ~20%.
Found it. It was last month.At any rate that person and a group of other docs/epidems were interviewed and after discussion they said the chances of another Omicron level event in the next 2-5 years was ~20%.
Do you recall roughly how long ago that was? Maybe the general consensus was more pessimistic in, say, mid-2022 versus today.
 erictopol.substack.com
erictopol.substack.com
I could see another Omicron peak happen if protection against severe disease drops off a cliff ...
 yourlocalepidemiologist.substack.com
yourlocalepidemiologist.substack.com
ACIP meeting: Spring booster Cliff notes
The ACIP meeting for spring boosters convened yesterday.
Once again ignoring people who actually got covid since the bivalent vaccines were introduced.ACIP meeting: Spring booster Cliff notes
The ACIP meeting for spring boosters convened yesterday.
Big takeaway:
Bottom line upfront
CDC and FDA are trying to simplify COVID-19 vaccine recommendations. (Verdict is out if they actually did this for kids). From now on, people are “up-to-date” if:
- 6+ years old: 1 bivalent (i.e. fall Omicron vaccine) dose. Regardless of vaccine history. Period.
- <6 years old:
- Moderna: at least 2 doses, including 1 bivalent.
- Pfizer:
- 5 years: 1 bivalent.
- Under 5 years: at least 3 doses, including 1 bivalent.
If you meet this criteria, there is nothing you need to do right now. You can stop reading.But this happens to be only 1 in 6 Americans (2 in 5 of those who 65 years and older). A ridiculous number of Americans are not up-to-date with COVID-19 vaccines. This means a lot of people need to keep reading.
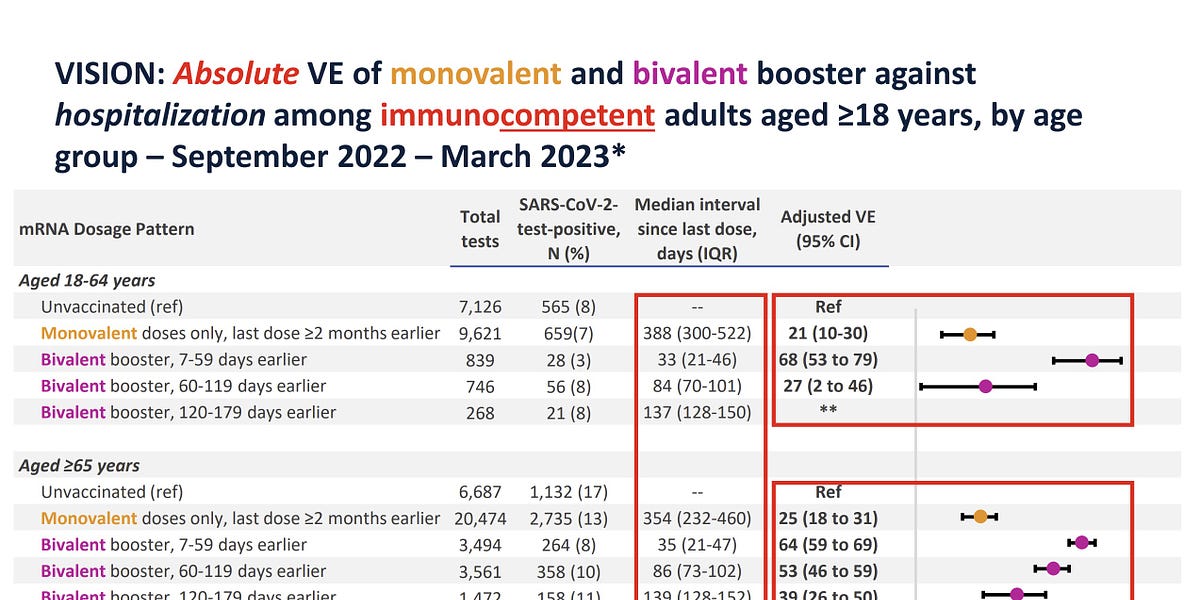
One thing I'd like to see a firm definition of what qualifies as "higher risk of severe COVID" (see charts in middle of YLE article).
- Getting the flu and COVID-19 vaccines simultaneously may be a problem. While not statistically significant, there is an elevated rate of stroke within 21 days. (It’s pretty darn close to being statistically significant, too.) I hope we get more clarity before the upcoming fall vaccine campaign.
ACIP meeting: Spring booster Cliff notes
The ACIP meeting for spring boosters convened yesterday.
Big takeaway:
Bottom line upfront
CDC and FDA are trying to simplify COVID-19 vaccine recommendations. (Verdict is out if they actually did this for kids). From now on, people are “up-to-date” if:
- 6+ years old: 1 bivalent (i.e. fall Omicron vaccine) dose. Regardless of vaccine history. Period.
- <6 years old:
- Moderna: at least 2 doses, including 1 bivalent.
- Pfizer:
- 5 years: 1 bivalent.
- Under 5 years: at least 3 doses, including 1 bivalent.
If you meet this criteria, there is nothing you need to do right now. You can stop reading.But this happens to be only 1 in 6 Americans (2 in 5 of those who 65 years and older). A ridiculous number of Americans are not up-to-date with COVID-19 vaccines. This means a lot of people need to keep reading.
One thing I'd like to see a firm definition of what qualifies as "higher risk of severe COVID" (see charts in middle of YLE article).
ACIP meeting: Spring booster Cliff notes
The ACIP meeting for spring boosters convened yesterday.
Big takeaway:
Bottom line upfront
CDC and FDA are trying to simplify COVID-19 vaccine recommendations. (Verdict is out if they actually did this for kids). From now on, people are “up-to-date” if:
- 6+ years old: 1 bivalent (i.e. fall Omicron vaccine) dose. Regardless of vaccine history. Period.
- <6 years old:
- Moderna: at least 2 doses, including 1 bivalent.
- Pfizer:
- 5 years: 1 bivalent.
- Under 5 years: at least 3 doses, including 1 bivalent.
If you meet this criteria, there is nothing you need to do right now. You can stop reading.But this happens to be only 1 in 6 Americans (2 in 5 of those who 65 years and older). A ridiculous number of Americans are not up-to-date with COVID-19 vaccines. This means a lot of people need to keep reading.
One thing I'd like to see a firm definition of what qualifies as "higher risk of severe COVID" (see charts in middle of YLE article).
Once again ignoring people who actually got COVID since the bivalent vaccines were introduced.
I read this post 3 times and I still don't understand what it is saying.ACIP meeting: Spring booster Cliff notes
The ACIP meeting for spring boosters convened yesterday.
Big takeaway:
Bottom line upfront
CDC and FDA are trying to simplify COVID-19 vaccine recommendations. (Verdict is out if they actually did this for kids). From now on, people are “up-to-date” if:
- 6+ years old: 1 bivalent (i.e. fall Omicron vaccine) dose. Regardless of vaccine history. Period.
- <6 years old:
- Moderna: at least 2 doses, including 1 bivalent.
- Pfizer:
- 5 years: 1 bivalent.
- Under 5 years: at least 3 doses, including 1 bivalent.
If you meet this criteria, there is nothing you need to do right now. You can stop reading.But this happens to be only 1 in 6 Americans (2 in 5 of those who 65 years and older). A ridiculous number of Americans are not up-to-date with COVID-19 vaccines. This means a lot of people need to keep reading.
One thing I'd like to see a firm definition of what qualifies as "higher risk of severe COVID" (see charts in middle of YLE article).
Also, this
I read this post 3 times and I still don't understand what it is saying.
Except she did take a positionOnce again ignoring people who actually got COVID since the bivalent vaccines were introduced.
Someone in her position is never, ever, going to say something like "Since you had COVID in the spring, you don't need a COVID booster in the fall". That's not how flu vaccination recommendations work, either. Recommendations for an annual prophylactic vaccine (so far as I'm aware) is always once-a-year like clockwork, infections notwithstanding.
@Terminalxylem , @gianmarco -- inviting your input on this point.
- What if I just had an infection? The CDC is still not providing recommendations based on infection history. (I was surprised.) Canada took this route, which I agreed with.
What are the current recommendations for vaccine boosters?I read this post 3 times and I still don't understand what it is saying.
Ask away.
What is Canada's route?Except she did take a positionOnce again ignoring people who actually got COVID since the bivalent vaccines were introduced.
Someone in her position is never, ever, going to say something like "Since you had COVID in the spring, you don't need a COVID booster in the fall". That's not how flu vaccination recommendations work, either. Recommendations for an annual prophylactic vaccine (so far as I'm aware) is always once-a-year like clockwork, infections notwithstanding.
@Terminalxylem , @gianmarco -- inviting your input on this point.
- What if I just had an infection? The CDC is still not providing recommendations based on infection history. (I was surprised.) Canada took this route, which I agreed with.
No idea.What is Canada's route?Except she did take a positionOnce again ignoring people who actually got COVID since the bivalent vaccines were introduced.
Someone in her position is never, ever, going to say something like "Since you had COVID in the spring, you don't need a COVID booster in the fall". That's not how flu vaccination recommendations work, either. Recommendations for an annual prophylactic vaccine (so far as I'm aware) is always once-a-year like clockwork, infections notwithstanding.
@Terminalxylem , @gianmarco -- inviting your input on this point.
- What if I just had an infection? The CDC is still not providing recommendations based on infection history. (I was surprised.) Canada took this route, which I agreed with.
What are the current recommendations for vaccine boosters?I read this post 3 times and I still don't understand what it is saying.
Ask away.
No idea.What is Canada's route?Except she did take a positionOnce again ignoring people who actually got COVID since the bivalent vaccines were introduced.
Someone in her position is never, ever, going to say something like "Since you had COVID in the spring, you don't need a COVID booster in the fall". That's not how flu vaccination recommendations work, either. Recommendations for an annual prophylactic vaccine (so far as I'm aware) is always once-a-year like clockwork, infections notwithstanding.
@Terminalxylem , @gianmarco -- inviting your input on this point.
- What if I just had an infection? The CDC is still not providing recommendations based on infection history. (I was surprised.) Canada took this route, which I agreed with.
| Susan Scheid 3 hr ago Thanks, as always, for the clear, concise summation. Two questions: For those of us over 65+ who have had recent infections, you note you agree with Canada’s approach. Van you advise what that is, and specifically, what waiting period is recommended? Re the stroke issue related to taking the flu and Covid vaxes at the same time, have you any sense of when the CDC will have guidance on this, and is there or will there be any recommendation as to how far apart and in what order the two vaxes should be taken? |
Katelyn Jetelina 3 hr agoAuthor These are good questions. 1. I meant to link the Canada policy, but forgot! Sorry. Here it is: https://www.canada.ca/en/public-hea...ls-high-risk-severe-illness-due-covid-19.html Basically they said everyone over the age of 80 needs a vaccine (regardless of infection status). For those 65-79 years old, they don't need a Spring booster if they EVER had an infection because hybrid immunity is showing to last at least 12 months. They didn't provide a time frame, because I don't think we know. So, I always use the 6 month rule. 2. During the CDC meeting, the scientists said they were confident there wasn't a safety signal. I was surprised not much was discussed about this, because usually we don't only rely on statistics, especially when it's so close to being significant. They did say they are looking into other data sources to try and understand this better. |
They probably use the CDCs list of high risk conditions
One thing I'd like to see a firm definition of what qualifies as "higher risk of severe COVID" (see charts in middle of YLE article).
You are correct. It's a little trickier with covid than flu though, as it hasn't established clear seasonality yet. And the overall potential for mutation is higher, despite the SARS-CoV-2 mutation rate being slower than influenza.Once again ignoring people who actually got COVID since the bivalent vaccines were introduced.
Someone in her position is never, ever, going to say something like "Since you had COVID in the spring, you don't need a COVID booster in the fall". That's not how flu vaccination recommendations work, either. Recommendations for an annual prophylactic vaccine (so far as I'm aware) is always once-a-year like clockwork, infections notwithstanding.
@Terminalxylem , @gianmarco -- inviting your input on this point.
According to Worldometers and using 7-day average, the U.S. was below 300 deaths/day from June 28 through July 14, 2021, with a low of 247 on July 8th. Of course, deaths lagged cases: from June 5 through July 2, 2021, the U.S. 7-day average for cases remained below 15,000 with a low of 12,093 on June 21.https://twitter.com/DiseaseEcology/status/1483958728709722114
What is an "acceptable" # of COVID-19 deaths in US? Lots of folks suggesting that post-omicron we can pretend we're post-pandemic. But 1K deaths/d = 365K deaths/yr Flu avg is ~35K/yr We need avg ~100deaths/day to get near flu We've never had daily avg <225 since Mar 2020
Idk if that's accurate but if not, it's probably pretty close. I think we were close to that last summer. But were we are again, back up in the 2-3K deaths per day range.
If those levels ever came back, and stayed sustained over several months in a row with maybe only some small regional bumps ... I would bet American society would more or less collectively turn the page.
Which map are you finding that on? I was looking at Daily Deaths, but I can't make that one produce your 590 number for 1/15 or the 150 for 4/12.(Old post from 1/25/2022):
According to Worldometers and using 7-day average, the U.S. was below 300 deaths/day from June 28 through July 14, 2021, with a low of 247 on July 8th. Of course, deaths lagged cases: from June 5 through July 2, 2021, the U.S. 7-day average for cases remained below 15,000 with a low of 12,093 on June 21.https://twitter.com/DiseaseEcology/status/1483958728709722114
What is an "acceptable" # of COVID-19 deaths in US? Lots of folks suggesting that post-omicron we can pretend we're post-pandemic. But 1K deaths/d = 365K deaths/yr Flu avg is ~35K/yr We need avg ~100deaths/day to get near flu We've never had daily avg <225 since Mar 2020
Idk if that's accurate but if not, it's probably pretty close. I think we were close to that last summer. But were we are again, back up in the 2-3K deaths per day range.
If those levels ever came back, and stayed sustained over several months in a row with maybe only some small regional bumps ... I would bet American society would more or less collectively turn the page.
Today, on Thur 4/27/2023, using 7-day averages:
- - The U.S. has been below 300 COVID deaths/day, sustained, since March 7, 2023
- - The U.S. has been below 200 COVID deaths/day, sustained, since April 8, 2023
- - The U.S. has been below 150 COVID deaths/day, sustained, since April 12, 2023
As a point of comparison, the 2023 high was 590 on January 15, 2023. The downwards slide since then has been consistent.
Which map are you finding that on? I was looking at Daily Deaths, but I can't make that one produce your 590 number for 1/15 or the 150 for 4/12.
Not supported whatsoeverDr. Aseem Malhotra tells Joe Rogan that a reanalysis of Pfizer and Moderna's original clinical trial data shows that their COVID mRNA vaccines *INCREASE* your risks of serious adverse events, hospitalization, and death: "In my whole career, looking at all of the drugs and knowing about many different prescribed medications, I've never seen something that when you look at the data has such poor effectiveness and unprecedented harms. In the summer of last year, in the journal Vaccine, the highest-impact medical journal for vaccines, they published a reanalysis of Pfizer and Moderna's original double-blinded randomized controlled trial. This is the highest quality of scientific evidence. Joseph Fraiman is an ER doctor and clinical data scientist from Louisiana. Associate editor of the BMJ, Dr. Peter Doshi. Dr. Robert Kaplan from Stanford. Some real eminence of integrity published this reanalysis, and what they found was this. In the trials that led to the approval of regulators worldwide, you were more likely to suffer a severe adverse event from taking the vaccine, hospitalization, disability, or life-changing event than you were to be hospitalized with COVID. This mRNA vaccine should likely have never been approved for a single human in the first place, and that rate of serious adverse events is at least 1 in 800... 1 in 800 is a very, very high figure. We've pulled other vaccines for much less. The 1976 Swine Flu vaccine was pulled because it was found to cause a debilitating neurological condition called Guillan-Barre syndrome in about 1 in 100,000 people. The Rotavirus vaccine was suspended in 1999 because it was found to cause a form of bowel obstruction in kids in 1 of 10,000. This is at least 1 in 800. It's a no-brainer. So the question is, why have we not paused it?"
Debunked as usualDr. Aseem Malhotra tells Joe Rogan that a reanalysis of Pfizer and Moderna's original clinical trial data shows that their COVID mRNA vaccines *INCREASE* your risks of serious adverse events, hospitalization, and death: "In my whole career, looking at all of the drugs and knowing about many different prescribed medications, I've never seen something that when you look at the data has such poor effectiveness and unprecedented harms. In the summer of last year, in the journal Vaccine, the highest-impact medical journal for vaccines, they published a reanalysis of Pfizer and Moderna's original double-blinded randomized controlled trial. This is the highest quality of scientific evidence. Joseph Fraiman is an ER doctor and clinical data scientist from Louisiana. Associate editor of the BMJ, Dr. Peter Doshi. Dr. Robert Kaplan from Stanford. Some real eminence of integrity published this reanalysis, and what they found was this. In the trials that led to the approval of regulators worldwide, you were more likely to suffer a severe adverse event from taking the vaccine, hospitalization, disability, or life-changing event than you were to be hospitalized with COVID. This mRNA vaccine should likely have never been approved for a single human in the first place, and that rate of serious adverse events is at least 1 in 800... 1 in 800 is a very, very high figure. We've pulled other vaccines for much less. The 1976 Swine Flu vaccine was pulled because it was found to cause a debilitating neurological condition called Guillan-Barre syndrome in about 1 in 100,000 people. The Rotavirus vaccine was suspended in 1999 because it was found to cause a form of bowel obstruction in kids in 1 of 10,000. This is at least 1 in 800. It's a no-brainer. So the question is, why have we not paused it?"
blah blah blahDebunked as usualDr. Aseem Malhotra tells Joe Rogan that a reanalysis of Pfizer and Moderna's original clinical trial data shows that their COVID mRNA vaccines *INCREASE* your risks of serious adverse events, hospitalization, and death: "In my whole career, looking at all of the drugs and knowing about many different prescribed medications, I've never seen something that when you look at the data has such poor effectiveness and unprecedented harms. In the summer of last year, in the journal Vaccine, the highest-impact medical journal for vaccines, they published a reanalysis of Pfizer and Moderna's original double-blinded randomized controlled trial. This is the highest quality of scientific evidence. Joseph Fraiman is an ER doctor and clinical data scientist from Louisiana. Associate editor of the BMJ, Dr. Peter Doshi. Dr. Robert Kaplan from Stanford. Some real eminence of integrity published this reanalysis, and what they found was this. In the trials that led to the approval of regulators worldwide, you were more likely to suffer a severe adverse event from taking the vaccine, hospitalization, disability, or life-changing event than you were to be hospitalized with COVID. This mRNA vaccine should likely have never been approved for a single human in the first place, and that rate of serious adverse events is at least 1 in 800... 1 in 800 is a very, very high figure. We've pulled other vaccines for much less. The 1976 Swine Flu vaccine was pulled because it was found to cause a debilitating neurological condition called Guillan-Barre syndrome in about 1 in 100,000 people. The Rotavirus vaccine was suspended in 1999 because it was found to cause a form of bowel obstruction in kids in 1 of 10,000. This is at least 1 in 800. It's a no-brainer. So the question is, why have we not paused it?"
And part of the article directly addressing this:
Reanalysis of clinical trial data from Pfizer and Moderna
One of the main pieces of evidence in the article is a study published by Fraiman et al. in the journal Vaccine[1]. In it, the authors analyzed data from a previous study of adverse events reported in the clinical trials of the Pfizer-BioNTech and Moderna mRNA COVID-19 vaccines[2,3]. They concluded that “The excess risk of serious adverse events of special interest was higher than the risk reduction for COVID-19 hospitalization relative to the placebo group” in both Pfizer and Moderna trials.
To arrive at this conclusion, the authors calculated how many more serious adverse events occurred in the vaccinated group compared to the control group. They then compared this figure with the number of people hospitalized with COVID-19 during the clinical trials.
To determine what kind of adverse events would be considered as serious for the purposes of the study, the authors looked to the Priority List of COVID-19 Adverse events of special interest by the Brighton Collaboration (BC), a program of the nonprofit organization The Task Force for Global Health. This list includes adverse events that have been seen with COVID-19, as well as those with a proven or theoretical association with vaccines in general or with specific vaccine platforms.
The now-published study was initially available as a preprint—a manuscript that hasn’t undergone peer review—in June 2022. Health Feedback previously reviewed it and found that the authors’ analysis didn’t support their conclusion. Scientists such as surgeon and cancer researcher David Gorski, biostatistician Jeffrey S. Morris, and nanomedicine expert Susan Oliver pointed out several issues in the study that indicated potential p-hacking.
P-hacking (also known as data dredging or data snooping) is the manipulation of data analysis to make the results look statistically significant when they aren’t. The study by Fraiman et al. showed several signs suggesting that the authors had analyzed data in a manner that favored their hypothesis.
First, the Brighton document lists “adverse events of special interest” (AESI) mainly as specific clinical diagnoses, such as enteritis/colitis, arthritis, and encephalitis. In order for the authors to count the number of serious AESIs associated with COVID-19 vaccines, they needed to determine which serious adverse events (SAEs) recorded in the vaccines’ clinical trials corresponded to the AESIs listed in the Brighton document.
The decision of whether an SAE corresponded to a Brighton AESI rested on the opinion of two independent clinicians, and a third one if the first two disagreed without arriving at a consensus.
However, the reasons for considering certain SAEs as corresponding to the AESI list are unclear and inconsistent. For example, one Brighton AESI is enteritis/colitis, for which the corresponding adverse events would be diarrhea and vomiting. However, the authors included diarrhea but not vomiting when counting relevant SAEs. Another example is the authors’ inclusion of arthritis as a serious adverse event, but not osteoarthritis (a form of arthritis).
The authors also excluded “events related to COVID-19”. While this exclusion could make sense when focusing on potential side effects of the COVID-19 vaccines, it introduces an important bias by eliminating adverse events that are expected to be much more common in the control group than in the vaccinated group. This means that the study was less able to detect harms from COVID-19. Overall, these observations suggest that the adverse events that the authors chose to analyze were the result of cherry-picking.
Second, the authors compared the people hospitalized with COVID-19 with the total number of adverse events in the control and the vaccinated groups rather than the number of individuals who reported the adverse events. Since one person can suffer multiple adverse events but only one hospitalization, this analysis leads to an overcounting of adverse events and over-represents the harmful effects of vaccination compared to the risks of COVID-19. For example, a person who reported colitis, diarrhea, and abdominal pain, would be counted as three adverse events, even though the three occurred in the same person and are likely related.
Finally, some of the included adverse events, such as diarrhea, abdominal pain, and rash, aren’t equivalent to a COVID-19 hospitalization in terms of disease severity. This analysis also doesn’t take into account the benefits of vaccination in preventing COVID-19 complications other than hospitalization, including cardiovascular problems.
Given the methodological flaws in the study, the analysis is unreliable and doesn’t support the claim that vaccines cause more serious adverse events than the benefits they provide.

That’s terrible, considering the potential for aerosolized fecal matter during that procedure.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
Yeah in many doctor/hospital settings I could see wearing a mask for sure.That’s terrible, considering the potential for aerosolized fecal matter during that procedure.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
Lmao I'm not talking about DURING the procedureThat’s terrible, considering the potential for aerosolized fecal matter during that procedure.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
Well then that first post was a bit misleading.Lmao I'm not talking about DURING the procedureThat’s terrible, considering the potential for aerosolized fecal matter during that procedure.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
I hope you don't remember the actual procedure. Lol. When I had one I told the nurse that gave me the drugs to put you in "twilight land" or whatever that "I was a bigger dude and she was probably gonna need to double that dose up." She just laughed at me and we started turning the corner to go down the hallway to the OR. The next thing I know I woke up in recovery. Just the way I WANTED to remember that procedure.Lmao I'm not talking about DURING the procedureThat’s terrible, considering the potential for aerosolized fecal matter during that procedure.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
 yourlocalepidemiologist.substack.com
yourlocalepidemiologist.substack.com
I was just at the doctor yesterday for my annual check-up. Everybody who was actually interacting directly with patients (my doctor, her nurse, the guy who drew my blood) were wearing masks. Almost nobody else was, including the receptionists. There were just a single-digit number of masked patients, but I have no idea what's up with those folks -- for all I know they're actually sick and contagious and/or immunocompromised somehow, and of course it makes sense for those people to mask up when they come in for care.When I got my colonoscopy at hospital two weeks ago nobody was wearing masks including doctors and nurses
 you guys really thought he meant during the procedure too?
you guys really thought he meant during the procedure too?